Primary care requesting patterns for estimated glomerular filtration rate and compliance with NICE chronic kidney disease guidelines
What is chronic kidney disease?
Chronic kidney disease (CKD) is defined as abnormalities of kidney structure or function lasting for at least 3 months, with adverse clinical consequences1. It is difficult to detect at early stages since the majority of patients are asymptomatic. A small but significant percentage of cases potentially progress to end-stage renal disease (ESRD) regardless of the underlying pathophysiological cause. CKD is a significant cause of mortality and morbidity, and escalating health costs related to cardiovascular disease and renal replacement therapies.
Diagnosis and monitoring of CKD is crucial in preventing or delaying development of ESRD, reducing occurrences of complications and, importantly, lessening the burden on the health care budget.
What are the tests for the diagnosis and monitoring of CKD?
Detection and monitoring can easily be achieved using simple tests such as an estimated glomerular filtration rate (eGFR) calculation in conjunction with serum creatinine and urine albumin creatinine ratio (ACR).
The serum and urine creatinine results, in our audit, were obtained using the Jaffé method (which is calibrated against isotope dilution mass spectrometry (the reference method)) as well as urine albumin using immunoturbidimetry. eGFR calculation, in our laboratory, is still based on the 4-variable Modification of Diet in Renal Disease (MDRD) equation.
NICE CKD classification & recommendations for follow up
In 20121, Kidney Disease: Improving Global Outcomes (KDIGO) guidance on the evaluation and management of CKD, stratified CKD according to eGFR (Grade 1 to Grade 5) and ACR (Grade 1 to Grade 3). According to this, decreased eGFR and increased ACR indicate increased risk of adverse outcomes in the disease process. Further to that, in 2015, NICE updated their guidance (CG182) on identification and investigation of individuals with CKD including frequency of monitoring of eGFR in each CKD category2.
What did Viapath audit?
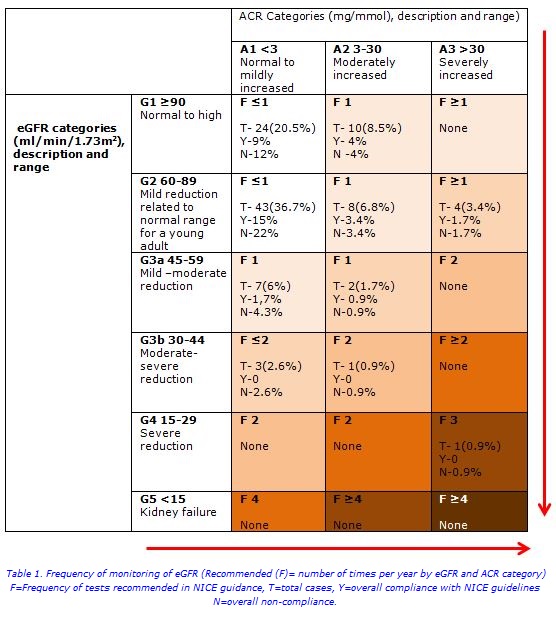
In our retrospective audit, we focused on adult requests from primary care to Viapath’s Clinical Biochemistry laboratory, King’s College Hospital, for eGFR and/or ACR for 2 months from January 2017. Frequency of monitoring of eGFR and ACR was determined over a one-year period for each patient and compared with NICE recommendations (Table 1).
Compliance of primary care for NICE recommendations
A total of 117 patients (55 males), aged 58 (±14) [mean (±SD)] years were categorised according to CKD grades as in table 1. The majority of patients, 43 (36.7%), were found in the G2A1 CKD category with mild reduction of eGFR and normal to mildly increased ACR.
The second common category for monitoring in Primary Care was A1G1 (24 cases: 20.5%). Interestingly, none of the patients from our cohort belonged to either the G1A3, G3aA3, G3bA3, G4A1, G4A2 or the eGFR kidney failure categories. Only ACR was requested in 14 (12%) cases within one year.
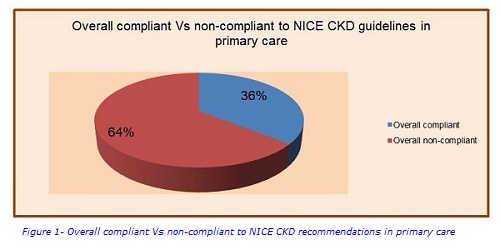
The overall compliance of monitoring CKD with NICE guidance in this study group was seen only in 42 (36%) cases whilst 75 (64%) cases were non-compliant.
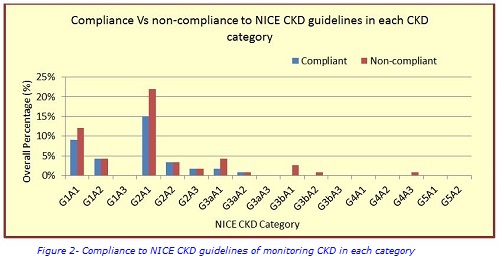
Compliance of monitoring of CKD with NICE recommendations in each category as a percentage to the total number of patients was demonstrated in both table 1 and figure 2.
Conclusions
In summary, it was found that CKD monitoring was not adequately performed in line with NICE recommendations. Over requesting occured at lower CKD grades (Grade 1-2) and under requesting occured at higher CKD grades (Grades 3-4). There is some evidence found in literature that eGFR graphs help to identify patients with deteriorating renal function earlier3. Early diagnosis of CKD has been advanced notably since nationwide introduction of eGFR reporting in the primary care Quality and Outcomes Framework as well as increased public and health care professional awareness of CKD. Nevertheless, despite all these measures, overall 19% of cases were still identified as late presentations according to the Renal Registry report issued by Renal Association, UK in 2013.
The laboratory can become the key link in engaging primary care and renal physicians to develop effective local policies for monitoring CKD.
For further information, please contact
Ruvini Ranasinghe
ruvini [dot] ranasinghe [at] nhs [dot] net
Anil Simhadri
anil [dot] simhadri [at] nhs [dot] net
Nandini Rao
nandinirao [at] nhs [dot] net
References
1.National Kidney Foundation. KDIGO 2012 Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013;3:1-50.
2.National Institute of Health and Care Excellence. Clinical guideline for Chronic kidney disease in adults: assessment and management (CG182). NICE 2017 2014;1-63.
3.Barton AL et al. The Cornish experience of the ASSIST-CKD project. Ann Clin Biochem 2018; 55(1):100-106.